
 Pregnancy Due Date Calculator
Pregnancy Due Date Calculator
 Chinese Gender Predictor
Chinese Gender Predictor
 Ovulation Calculator
Ovulation Calculator
 IVF Due Date Calculator
IVF Due Date Calculator
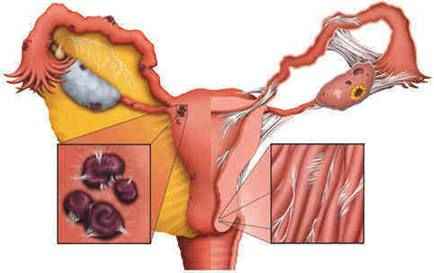
Endometriosis
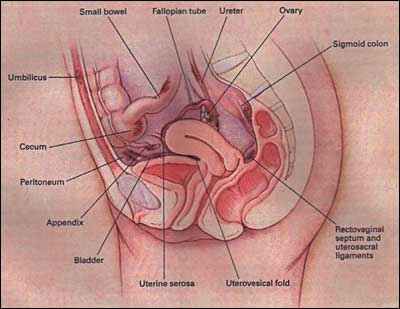
It is a condition where pieces of the endometrium grow outside the uterus, most commonly in the ovaries, Fallopian tubes, bowel, and bladder, and rarely travel far from the pelvic region into the lung, skin, and other regions of the body, but it is a non-cancerous condition.
Fallopian tubes, bowel, and bladder, and rarely travel far from the pelvic region into the lung, skin, and other regions of the body, but it is a non-cancerous condition.
This tissue continues to respond to hormonal signals, specifically estrogen from the ovaries each month which stimulate it to grow, and when the estrogen level drops, the tissue bleeds, after which an inflammatory process and adhesions occur. With each period, we expect blood to collect and form a chocolate cyst of the ovary.
This disease affects 10-15% of premenopausal women, and it is a common cause of pelvic pain and infertility. About 35-50% of women with this disease have difficulty in getting pregnant due to adhesions, altered prolactin release, oocyte maturation defects, and anovulation.
Symptoms of Endometriosis:
 1- The most common symptom is painful menstrual cycles.
1- The most common symptom is painful menstrual cycles.
2- Dyspareunia
3- Menorrhagia
4- Pelvic pain and backache
5-Dyschesia & rectal bleeding in cases of colonic endometriosis
6- Nausea & vomiting and abdominal cramps in endometriosis of the small intestine
7- Hematuria and frequency in endometriosis of the urinary bladder
Causes of Endometriosis:
Causes of this disease are still unknown, but some researchers believe endometriosis is due to an immune system problem or hormonal imbalance. Others believe endometriosis is a genetic condition. Studies found an increased risk (5-7%) in women with family history of this disease.
Theories of causation of Endometriosis include:-
· Retrograde menstruation
· Lymphatic and vascular dissemination
· Coelomic metaplasia
Stages of endometriosis:
 We have four stages for this disease.
We have four stages for this disease.
1-Microscopic endometriosis: In this stage, the peritoneum appears normal macroscopically, and lesions are identified using electron microscopy. The endometrial deposits contain endometrial gland and stroma.
2-Early active endometriosis:
It appears as vesicles, papules; maybe solid or fluid-filled and highly vascular and non-fibrotic-containing glands in the proliferative or secretory phase.
3-Advanced active endometriosis:
Present as pigmented hemorrhagic and fibrotic endometriotic deposits known as classic lesions.
4-Healed endometriosis:
Appears as white nodules or flattened fibrotic scar-containing glands only.
Risk factors for Endometriosis:
. Japanese race
. Family history
. Age 30 – 44 years
. Alcohol – caffeine intake
. Increased peripheral fat
Prevention of Endometriosis:
There is no known way to prevent this disease, but some believe women having more than one child and having children early in life develop a certain level of protection against the disease and women with a long-term use of birth control pills are less likely to develop endometriosis.
Complications of Endometriosis:
1- Infertility
2- Intestinal obstruction
3- Ureteric obstruction
4- Secondary infection of the endometriotic lesions
5- Rupture of endometrioma.
Investigations of Endometriosis:
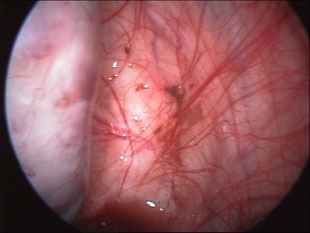
1- Laparoscopy : - considered the gold standard when endometriosis is suspected. 50% of women with pelvic pain and dysmenorrhoea have endometriosis diagnosed at laparoscopy.
2- Ultrasonography : - have limited value in the diagnosis of endometriosis but is helpful when there is an endometrioma.
3- MRI: - detects endometrioma, ovarian adhesions, and extra peritoneal masses and detects invasion to bowel, bladder, and rectovaginal septum.
4- Blood test CA 125: This protein increases in patients with severe endometriosis but also increases in ovarian cancer and peritonitis. It is not a sensitive test since it cannot detect the disease in early stages, and it is not specific, but can be used for followup in treated patients to check their response to treatment.
Treatment of Endometriosis:
There is no definite cure for this disease, but several options are available.
Medical Treatment of Endometriosis
. (NSAIDS) non- steroidal anti- inflammatory drugs such as ibuprofen are helpful in reducing the severity of dysmenorrhoea.
. Combined oral contraceptive pills
Three packs of pills taken continuously are helpful in decreasing the number and frequency of the menstrual cycles, thus causing atrophy of the endometriotic spots.
. Progestogen
Such as medroxyprogesterone given continuously will produce pseudo-decidualization in endometriotic lesions, but has the side effects of weight gain and breakthrough bleeding along with the mood swings.
. Danazol
This drug has androgenic effect and is given in the dose 400-800 mg daily for three to six months, but it has the side effects of acne, weight gain, and hirsutism.
. GnRH agonists
Present as nasal spray, subcutaneous, or intramuscular injection. These drugs cause down-regulation of pituitary function, which suppresses ovarian steroid production and induces pseudo-menopause. Their side effects include hot flushes, atrophic vaginitis, and bone pain unless they are given with hormone replacement therapy as ADD-BACK THERAPY. Studies found that GnRH agonists given for endometriosis patients undergoing in-vitro fertilization cycles improve significantly their fertility and decreases preclinical abortions.
Surgical Treatment of Endometriosis
The surgery aims to palliate symptoms, increase fertility, remove endometriotic implants, and delay recurrence of the disease.
Conservative surgery done with laparoscopy is a diagnostic as well as a therapeutic procedure used to remove endometriotic lesions by laser or diathermy and adhesolysis. This type of treatment reduces the need for open surgery in young women who seek future pregnancies.
Radical surgery
This is reserved for cases with severe symptoms and progressive disease or women who have completed their families. Such procedures include hysterectomy and bilateral salpingo – oophorectomy. Nearly 12% of all endometriosis patients require radical surgery.
Endometriosis surgery is more effective in treating severe cases than a mild or minimal disease.
Surgery in minimal or mild disease fails to restore normal fertility.
Endometriosis and Assisted reproduction techniques:-
Endometriosis patients with long-term infertility can benefit from assisted reproduction techniques in overcoming their infertility.
Studies have shown that pretreatment with LH RH – analogues are associated with better fertilization and implantation results, especially in severe forms. Higher IVF pregnancy rates are found when there is a six-month pre-treatment using LH RH analogues and their effects seem to be more important for ovarian than endometrial level.
In cases of mild and moderate endometriosis with normal findings at salpingoscopy, (GIFT) can be a useful option, but some studies have noted that the results are less encouraging after GIFT than after IVF or ICSI.
In endometriosis, there is a risk for spontaneous abortion.
Abortion rates are 11.7% in mild endometriosis and 13.6% in moderate forms of the disease regardless of the stimulation protocol used.
Abortion rates of 60% in severe endometriosis cases were noted when there was no pretreatment using LH RH agonists.
Endometriosis in menopause
Post-menopausal endometriosis is one of the most unusual facets of endometriosis. It is found in 5% of menopausal women, more often in the years immediately following the menopause.
Clinical presentations:-
-Metrorrhagia
-If you find the enlarged uterus which may be fixed, it raises the suspicion of endometrial cancer.
-Pelvic mass
The association of post-menopausal endometriosis and neoplasia is possible. The transformation of an endometriotic lesion to malignancy occurs in 0.7-1% mostly on the ovary, but can also take place in the recto vaginal septum and colon.
Causes:-
Active endometriosis
It indicates that estrogens are still being produced in the body or are supplied exogenously as in cases of:
1- Women on HRT.
2- Patients taking Tamoxifen.
3- Obese women in whom peripheral androgens are converted to estrogens.
4- Secretory ovarian tumors.
Hormone-independent endometriotic lesions in which the receptor level is much lower in the lesion than in the endometrium and not influenced by hormonal variation as the endometrium, so it gives rise to severe and extensive clinical forms requiring hysterectomy with castration along with cyclic progestogen for six months, then estrogen – progestogen cyclic therapy.
Dr Najeeb Layyous F.R.C.O.G
Consultant Obstetrician, Gynecologist and Infertility Specialist